Announcement: Volunteer Opportunities for Paediatricians, Medical and Pre-Med Students at Chisang Clinic in rural eastern Nepal
With a growing patient load of newly born, toddlers and small children and an increase in ANC and PNC services, Chisang Clinic seeks Paediatricians, Medical and Nursing Students, and Pre-Med Student volunteers for 2014.
Please contact Chisang Clinic at chisangclinic@gmail.com for more information on this new volunteer position.
Announcement: Volunteer Opportunities for OB/GYN, Medical and Pre-Med Students at Chisang Clinic in rural eastern Nepal
Equipped with a clinic-based and portable USG, a fully functional Path Lab and ever increasing caseload of pregnant mothers, new mothers and women, both married and single, seeking OB/GYN services, Chisang Clinic seeks OB/GYN, Pre-Med and 4th and 5th year medical student volunteers for all of 2014.
Please contact Chisang Clinic at chisangclinic@gmail.com for more information on this new volunteer position.
Meghan and Chloe’s Experience at Chisang Clinic (Vol. II)
To conduct the feasibility study, a doctor from the United Kingdom came to the clinic and we set up a research team, with another nurse from Nepal, to write up a draft for all the considerations a birthing center would need. During the two weeks the doctor was at the clinic, we worked on bringing all the pieces together. We were lucky to have power 24 hours a day while at the clinic, but as there was no internet, frequent 45 minute bus rides to internet cafes became part of our routine. The project was both a learning experience for us, as well as a chance to both develop and plan for education for future patients of the clinic.
What we ended up creating was an outline with a variety of information and suggestions for future volunteers. It included an outline of clinical protocol, basic space and equipment needs, education material for patients, paperwork for clinical use and staffing needs. After it is finished, it will be submitted to the Nepali government for approval. Then work will begin on physically building the clinic and gathering supplies. While at the clinic, all construction efforts were focused on a second clinic being built in the hills north of Bhaunne. A full-time carpenter busily worked on furniture for the new building while we were there. So not only did we get to volunteer as nurses, but we also tried our hands at carpentry. The carpenter was nice enough to let us give bed-building a try.
Another skill we attempted to hone while at Chisang Clinic was cooking. The girls who take care of the volunteers made great food. We wanted to be able to impress our friends and families by learning their secrets, so they were kind enough to show us a few tricks. They even let us cook for them on Christmas morning. And to our surprise, everyone seemed to like it. We still have a ways to go when it comes to making Nepali food. However, what’s important is that we soaked up as many experiences as we could while we were there. And from the beginning, nursing was just one aspect of our trip to Nepal, the culture and the experiences we had outside our work left a much bigger impression on us.
Meghan and Chloe’s Experience at Chisang Clinic (Vol. I)
Meghan and I are nurses from University of Washington Medical Center in Seattle, Washington. We came to Nepal as first-time international volunteers. With the help of Village Volunteers, we were connected with the Chisang Clinic. After flying to Nepal, we stayed in Kathmandu for several days, then flew south to Biratnagar. We were greeted at the airport by Debendra Karki, the clinic’s founder, and taken to Bhaunne. Bhaunne is a small village in the southeastern part of the Terai. Because of it’s location, area is quite flat, and generally quite warm and humid. We lucked out because we came in the winter, so the nights were cool and foggy, and the days were warm and sunny. The village itself is fairly serene and pastoral. It is mainly agriculturally based, so there are many fields, and farms with animals. Behind the village is a tropical/sub-tropical rainforest with monkeys and a variety of birds. The village is far enough away from the highway to be quiet, but close enough, that after a quick walk, buses to bigger towns are readily accessible.
Although seemingly quite basic, and in some cases lacking by American standards, the people of the Morang district which Bhaunne is located in, actually enjoy the highest standard of living in Nepal. Every day we saw the children going to school, practicing good dental hygiene and eating dahl, bhaat, tarkari (rice, lentils and curried vegetables). However, for as many positive practices as we saw, while at the clinic, we got a chance to learn about a variety of gaps in education, as well as barriers to accessing healthcare in the community.
The majority of presenting complaints we saw at the clinic were rashes, viral infections, wounds, hypertension, and gynecological issues. For a variety of reasons, however, patients frequently do not follow up after their initial visits. Therefore the pace of the clinic was pretty slow. From getting a chance to meet some community members, as well as talking with Debendra, it became evident that there were many people who had health issues that were not being addressed. In some cases, it was due to poverty, in some cases it was lack of access to medical facilities with adequate means for intervention, and in some cases it was a lack of education.
A small example of the need for education was one woman who came into the clinic with her infant who had an ear infection. The child had had the infection for several days, and instead of seeking medical care, the woman had poured heated oil into the ear canal and inserted a chicken feather afterward to clean the opening out. When the infection did not clear, she brought the child in. In addition to treatment, she was given teaching on infection control and hygiene.
However, the goal of the Chisang Clinic is to move away from general practice, and focus solely on mothers and children. Nepal has one of the top ten highest infant and maternal mortality rates in the world. So to utilize our time at the clinic most effectively, we were asked by Debendra to conduct a feasibility study for the development of a birthing center.
Feasibility Study for Chisang Clinic Birthing Centre
Introduction:
Ever since Chisang Clinic Bhaunne was inaugurated in Mid-April 2012, the Clinic has been working hard to run a Well Child Clinic and a Well Woman Clinic between 10 AM and 2PM on different days of the week. Over the past few months, Chisang Clinic Bhaunne has been requested by the local Women’s Group to operate a Birthing Center to serve women from a 20 kil0meter radius. With small financial support from our past international volunteers and other individuals, Chisang Clinic is currently constructing the Birthing Center within the premises of Chisang Clinic Bhaunne. A Feasibility Study Team that included a physician from the UK, two nurses from Seattle, WA and a Nepali nurse, has worked for over two weeks to finalize this Feasibility Study for the Chisang Clinic Birthing Center.
Chisang Clinic
Guidelines for Birthing Centre Implementation
December 2012
Dania Bakhbakhi BMedSci MBChB DRCOG
Chloe Rahmun RN BSN
Meghan Young RN BSN
Sonal Bhattarai RN BSN
Background
- According to UNICEF, between 2006 and 2010, a Skilled Birthing Attendant is present at only 19% of births in Nepal. During this same time, only 18% of births were institutional deliveries.
- With the majority of women giving birth at home, the risks of both maternal and fetal morbidity and mortality are vastly increased.
- For the village of Bhaunne in the Morang district, the nearest hospitals are Koshi Zonal and B. P. Koirala Institute of Health Science.
- Koshi Zonal Hospital is in Biratnagar, and BPKIHS is in Dharan. Both hospitals are over an hour away from the community, making physical accessibility to medical care a challenge.
- Additionally, the average cost of a non-complicated delivery in Nepal is approximately $100-$600, which many people cannot afford.
Aim
Our aim is to establish a safe and sustainable birthing centre for the population of Bhaunne village and the surrounding area, in order to increase women’s accessibility to healthcare.
Organisational Considerations
Catchment Area: Bhaunne village and surrounding community of approximately 20 km diameter
Criteria for Admission to Birthing Centre
- Low risk pregnancies only
- Age 18-35
- Gestation 37-41 weeks
- No significant co-morbidities (See Table 1)
- No previous birthing complications (See Table 2)
- No previous caesarean sections
- No current pregnancy complications (See Table 3)
- Has been known to clinic from early pregnancy and has attended regular routine check ups
- No spontaneous attendances of women in labour. Advise to go straight to hospital in that case.
- Has had all the necessary blood tests and investigations e.g. full blood count, urea and electrolytes, and infection screening
- Patient should have been compliant with treatment prescribed
Table 1: Medical Conditions not permitted at Birthing Centre
|
Disease Area |
Medical Condition |
| Cardiovascular | Confirmed cardiac disease Hypertensive disorder |
| Respiratory | Asthma requiring an increase in treatment or hospital treatment Cystic fibrosis |
| Haematological |
|
| Infective |
|
| Immune | Systemic lupus erythematosus Scleroderma |
| Endocrine |
|
| Renal |
|
| Neurological | Epilepsy, Myasthenia gravis, Previous cerebrovascular accident |
| Gastrointestinal | Liver disease associated with current abnormal liver function tests |
| Psychiatric | Psychiatric disorder requiring current inpatient care |
| Gynaecological |
|
Table 2: Previous complications not permitted at birthing centre
| Previous complications |
|
Table 3: Current complications in pregnancy not permitted at birthing centre
| Current pregnancy and fetal indicaions |
|
Staff Qualifications
SBA training:
- 3 certified SBAs on staff at any given time
- Must be up to date with standardised skilled birthing attendant criteria
- Must be in compliance with all Nepali government SBA requirements
Workforce numbers:
- 3 to 4 skilled birthing attendants
- 1 Physician on call with 24 hour cover of the clinic e.g. O&G consultant
- Part-time ultrasound technician
- Interns, including USMLE candidates
- Housekeeper/ food prep
- 2 Nursing assistants
Shift rotations:
- More staff there may be required at different times of the year
- Use booking diary to predict busy times and to staff accordingly
Specific Training:
- Episiotomies
- Post partum haemorrhage
- Neonatal Resuscitation training
- Basic Life support training
- Breastfeeding training
- Patient education e.g. reducing infection, stool softeners, when stitches come out
Volunteers:
- Medical professionals e.g. doctors (O&G, GP, Sexual and reproductive health), midwives, labour and delivery nurses, nurse practitioners
- Students: observation, research and experience
- Flow and consistency: partnerships with Universities in Nepal, UK, US and worldwide, particularly ones with International Health programmes
Support groups:
- Find out more information about women support group
Equipment and Workspace
Building:
- Minimum of 300 x 15 square feet
- Western toilet and adequate bathing facilities for mother and baby
- 24 hour supply of clean and hot water and electricity supply (including emergency lighting)
- 24 hour refrigerator for storing medicines
- Equipment in satisfactory condition
- One patient bed per room must be adjustable and allow for gynaecological examination and delivery i.e. needs to have stirrups
- Opaque curtains and dividers to provide patient privacy for each room
- Each room must have it’s own adjustable bright lighting
- Oxygen tank and supply to the delivery room, must be secured to solid object
- Adequate prevention from occupational hazards
- No animals in the clinic
- All windows and doors should be covered with a minimum of a net covering
- Sufficient ventilation
- Absolutely no smoking on the premises with an obvious sign at front desk
Cleaning and sanitation:
- Daily thorough cleaning of facilities with the use of a regimented checklist
- Cleaning of individual patient areas after every use e.g. wiping down beds and cleaning up any spillage of body fluids
- Individual disposal bins for sharp equipment, clinical waste and household general waste with ideally a safe and environmentally friendly method of discard
- Sufficient plumbing and drainage facilities
- Hand washing sinks and alcohol gel to be located near clinical workstation
- A scrub room
- A dirty utility room for dirty linen and sanitary waste
- A clean linen closet and laundry bag
- A sterile laundry facility
- Adequate method of sterilisation of reusable instruments e.g. autoclave
- Thorough hand washing with water and soap before and after each and every patient contact including before and after each patient intervention or procedure
- Alcohol gel to be applied on entering and leaving the birthing centre
Sharps and Biohazard Disposal:
All sharps including needles, finger sticks, glass, ampules, IV supplies, and specimen containers will be disposed of in a puncture proof plastic container provided by the clinic. Each container when full will be disposed of in a 3 meter deep hole, at least 20 meters from the nearest water supply and building, as recommended by Where Women Have No Doctor. Biohazardous material including blood and birthing by-products should be disposed of via incineration, or disposed of by the same method as detailed above.
Equipment Needed and Predicted Cost:
Antenatal Equipment
| Item | Cost |
| Antenatal paperwork | |
| Gloves | |
| Alcohol gel | |
| Weighing scale | |
| Blood pressure monitor | |
| Blood glucose monitor | |
| Thermometer | |
| Ultrasound | |
| Doppler ultrasound | |
| Fetoscope | |
| Measuring tape | |
| Stethoscope | |
| KY lubricant | |
| Speculum | |
| Torch | |
| Tourniquet | |
| Needles | |
| Syringe | |
| Urine dipstick | |
| Sterile universal containers | |
| Gynaecology examination bed | |
| Examination lighting |
Equipment needed for delivery
| Item | Cost |
| Delivery Paperwork including partogram | |
| Long sterile gloves | |
| Sterile gown and mask | |
| Sterile or clean drapes | |
| Clean linen | |
| Birthing bed | |
| Examination lighting | |
| Vomit bowl | |
| Wipes | |
| Towels | |
| Soap | |
| Chlorhexidine wash | |
| Normal gloves | |
| Fetoscope | |
| Doppler ultrasound and gel | |
| Fetal heart monitor | |
| Ultrasound | |
| Stethoscope | |
| KY lubricant | |
| Speculum | |
| Torch | |
| Tourniquet | |
| Needles | |
| Syringe | |
| Urine dipstick | |
| Sterile universal containers | |
| IV cannulas ideally 18 gauge as a minimum | |
| Sterile saline flush | |
| Gauze | |
| IV fluids e.g. 0.9% NaCl, 5% Dextrose, Hartmans (500ml-1L) | |
| Drip stand or hook on wall | |
| Pulse Oximeter | |
| Oxygen masks, supply and tubing | |
| Two bowls to receive afterbirth |
Post-partum
| Item | Cost |
| Post natal paperwork | |
| Umbilical clamp | |
| Basic instrument pack | |
| Forceps | |
| Episiotomy scissors | |
| Kochers forceps | |
| Blankets | |
| Cot | |
| Hat | |
| Suction | |
| Blanket warmer | |
| Thermometer | |
| Sterile pad | |
| Blood glucose monitor | |
| Baby weighing scale | |
| Blood pressure monitor | |
| Pulse oximeter | |
| Suture | |
| Suture set | |
| Stitches cutter | |
| Paper towels | |
| Apron | |
| Gum boots | |
| Catheter | |
| Bed pan | |
| Bell | |
| Masks | |
| Emergency transport |
Medications
- Entonox
- Paracteamol
- Pethidine/opiods
- Non steroidal anti-inflammatories
- Antiemetics
- Anti Rh-D Immunoglobulin
- Oxytocin
- Vitamin K
- Broad spectrum antibiotics
- Erythromycin drops for eyes
- Albendazole
Emergency Vehicle
- 24 hour availability to allow prompt transfer to hospital, in case complications or complex care
Collaboration
- For transfer, partner with nearby hospitals: Koshi Zonal and BPKIHS
Business model and goals
Cost/benefit analysis:
- Cost of training
- Cost of care and supplies to patient
- Normal cost for delivery in Nepal:
- Aiming to cost around
- Cost of doctor
- Cost of staff
Clinical Considerations
Chisang Clinic Birthing Centre, Confidentiality Statement
At Chisang Clinic, our goal is to provide the best possible security and privacy measures for each patient. All patient reports, documents, lab values, and information will be kept confidential by the staff of Chisang Clinic. Prior to the release of any information, the patient will first be asked for permission to disclose sensitive material to external parties. Staff members not associated with the patient’s care unless required for quality improvement will not review records. All records will be kept for the duration of the patient’s life, after which time the records will be destroyed to protect confidentiality. All records will be kept in a locked, secure area of the clinic with no public access.
Antenatal Care
Patients should be given a choice at outset of care to have their birth at Chisang Clinic Birthing Center or in the hospital. They should be educated that if something goes wrong during their labour, outcomes for the woman and baby may be better in an obstetrics unit at hospital. Obstetric units may be able to provide direct access to obstetricians, anaesthetists, neonatologists and other specialised care, including epidural analgesia. At any point during pregnancy or delivery, they may need to be transferred to a hospital for emergency treatment.
Antenatal Guidelines
First Visit: When the mother first realizes she is pregnant
- Start antenatal packet (Appendix 1)
- Start antenatal flow chart (Appendix 2)
- Patient Screening Questionnaire (Appendix 3)
- Education for the Mother:
– How the baby develops during pregnancy – government poster
– General Advice About What to Expect During a Healthy Pregnancy (Appendix 4)
– Keeping Healthy While Pregnant (Appendix 5)
– Danger Signs During Pregnancy (Appendix 6)
- Laboratory Tests
– Hemoglobin
– Hepatitis B
– HIV: if positive, refer to Koshi Zonal Hospital, in Biratnagar, for follow up testing
– Blood glucose
– ABO blood group and antigen test
– Urine dip: for proteinuria
- Vitamin Supplementation and Medications
– Folic Acid 400 mcg per day until the 12th week of pregnancy: this helps prevent neural tube defects
– Iron supplements should not be offered routinely: give only if anaemic or hemoglobin <11g/100mL
– Multivitamins
- Antenatal prophylactic anti-D treatment for all women who are rhesus-D negative – check nepali guidelines
Second Visit: Between 18-20 Weeks
- Follow up with first visit and make sure patient has completed required tests.
- Continue to use Antenatal Flow Chart (Appendix 2) and record observations, VS, weight, fundal height, and any problems or concerns the expecting mother may have.
- Labs: Blood Glucose.
- Make plan for next visit.
Third Visit: Between 24-28 weeks
- Follow up with second visit
- Continue Antenatal Flow Chart (Appendix 2) and record observations, vital signs, weight, fundal height, and any problems or concern the expecting mother may have.
- Laboratory Tests:
– Haemoglobin
– Urine: proteinurea
– Blood glucose
– Oral Glucose Tolerance Test (OGTT)
- OGTT Guidelines Need to look up exact amounts and how often a women needs to come back for BG checks after diagnosis.
- Ultrasound
- Make plan for next visit.
Fourth Visit: Between 32-36 Weeks
- Follow up with third visit
- Continue with Antenatal Flow Chart (Appendix 2) and record observations, vital signs, weight, fundal height, and fetal presentation.
– If fetus is found to be malpositioned through palpation, a confirmation must be done by ultrasound.
– If it is confirmed by ultrasound, give the woman a choice to follow up in one to two weeks for a repeat ultrasound to check fetal position. If at that time the fetus is still malpositioned the woman should be referred to the nearest hospital and told she may not give birth at the clinic; however all post natal care from the 6 week baby check on are still available to her.
- Lab tests:
– Haemoglobin:
- Normal: >10.
- If haemoglobin <10, the woman should be referred to hospital for her birth, as low Hb signifies a greater probability of bleeding during birth and the possible need for blood products which the clinic cannot provide.
– Blood Glucose
– Urinalysis dipstick – protein check to rule out pre-eclampsia.
- Discuss upcoming delivery with the woman and go over any concerns or questions she may have.
- Encourage financial planning and discuss costs.
- Encourage prompt mobilization towards the birthing centre as soon as they feel the beginning stages of labour.
- Discuss the possibility that they may not be able to give birth at the clinic, should there any complications with their labour.
Other Visits
- Reasons for extra visits include, but are not limited to: high blood pressure, pain in abdomen, and extra blood sugar checks
- Other visits should be at the discretion of the patient and the SBA providing antenatal care
Intrapartum Care
- No contraindications for admission to birthing centre as outlined in Tables 1-3
- Admission only if in established labour
- Discuss birth plan e.g. relatives present, home food, own advocate during birth
- Sign consent form for admission to Chisang Clinic Birthing Centre (Appendix 7)
- Start Packet for Inpatient Delivery (Appendix 8)
First Stage of Labour
Definitions:
- Latent first stage of labour: A period of time, not necessarily continuous, when: there are painful contractions and some cervical change, including cervical effacement and dilatation up to 4 cm.
- Established first stage of labour: When there are regular painful contractions and progressive cervical dilatation from 4 cm.
Duration of the first stage labour:
- Nulliparous: 8-18 hours
- Multiparous: 5-12 hours
Assessment
Initial Assesment of a woman in labour should include:
- Listening to her story and review clinical records
- Physical observation: temperature, pulse, blood pressure, urinalysis
- Length, strength and frequency of contractions
- Abdominal palpation: fundal height, lie, presentation, position and station
- Vaginal loss: show, liquor, blood
- Assessment of pain
- FHR auscultated for a minimum of 1 minute immediately after a contraction
- Vaginal examination should be offered if woman is in established labour
Analgesia
- Breathing and relaxation techniques
- Entonox (50:50 oxygen and nitrous oxide)
- Pethidine or opioids
– May have side effects including nausea and vomiting and could respiratory depression or drowsiness in her baby
IV Fluid access
- 2 large cannulae (at least 18G/Green) to be inserted into a patient’s veins on admission
Assessment
- A pictorial record of labour (partogram) should be used once labour is established
- World Health Organization recommends 4-hour action line on partogram, should one be used
Observations (See Partogram: Appendix 9)
- Temperature and blood pressure every four hours
- Pulse every hour
- Documentation of frequency of contractions every thirty minutes
- Frequency of emptying the bladder
- Vaginal examination offered every four hours, or where there is concern about progress or in response to the woman’s wishes (after abdominal palpation and assessment of vaginal loss).
- Intermittent auscultation of the fetal heart after a contraction should occur for at least one minute, every fifteen minutes, and the rate should be recorded as an average. The maternal pulse should be palpated if a FHR abnormality is detected to differentiate the two heart rates. Intermittent auscultation can be undertaken by either Doppler ultrasound or Pinard stethoscope.
Second Stage of Labour
Definitions:
- Passive second stage of labour: The finding of full dilatation of the cervix prior to or in the absence of involuntary expulsive contractions.
- Onset of the active second stage of labour: The baby is visible with expulsive contractions and a finding of full dilatation of the cervix or other signs of full dilatation of the cervix. As well as active maternal effort following confirmation of full dilatation of the cervix in the absence of expulsive contractions.
Duration of the second stage labour
- Nulliparous: Birth would be expected to take place within 3 hours of the start of the active second stage in most women.
- A diagnosis of delay in the active second stage should be made when it has lasted 2 hours and women should be referred to a healthcare professional trained to undertake an operative vaginal birth if birth is not imminent.
- Multiparous: Birth would be expected to take place within 2 hours of the start of the active second stage in most women.
- A diagnosis of delay in the active second stage should be made when it has lasted 1 hour and women should be referred to a healthcare professional trained to undertake an operative vaginal birth if birth is not imminent.
Observations
- Blood pressure and pulse every hour
- Temperature every four hours
- Vaginal examination offered every hour in the active second stage or in response to the woman’s wishes (after abdominal palpation and assessment of vaginal loss)
- Documentation of the frequency of contractions every hour
- Frequency of emptying the bladder
- Ongoing consideration of the woman’s emotional and psychological needs.
- Assessment of progress should include maternal behaviour, effectiveness of pushing and fetal wellbeing, taking into account fetal position and station at the onset of the second stage. These factors will assist in deciding the timing of further vaginal examination and the need for obstetric review.
- Intermittent auscultation of the fetal heart should occur after a contraction for at least one minute, at least every five minutes. The maternal pulse should be palpated if there is suspected fetal bradycardia or any other FHR anomaly to differentiate the two heart rates.
- Ongoing consideration should be given to the woman’s position, hydration, coping strategies and pain relief throughout the second stage.
Women’s Position and Pushing in the Second Stage
- Women should be discouraged from lying supine or semi-supine in the second stage of labour and should be encouraged to adopt any other position that they find most comfortable.
- Women should be informed that in the second stage they should be guided by their own urge to push.
- If pushing is ineffective or if requested by the woman, strategies to assist birth can be used, such as support, change of position, emptying of the bladder and encouragement.
Reducing Perineal Trauma
- Perineal massage should not be performed by healthcare professionals in the second stage of labour.
- Either the ‘hands on’ (guarding the perineum and flexing the baby’s head) or the ‘hands poised’ (with hands off the perineum and baby’s head but in readiness) technique can be used to facilitate spontaneous birth.
- Lidocaine spray should not be used to reduce pain in the second stage of labour.
- A routine episiotomy should not be carried out during spontaneous vaginal birth.
- Where an episiotomy is performed, the recommended technique is a mediolateral episiotomy originating at the vaginal fourchette and usually directed to the right side. The angle to the vertical axis should be between 45 and 60 degrees at the time of the episiotomy.
- An episiotomy should be performed if there is a clinical need such as instrumental birth or suspected fetal compromise.
- Tested effective analgesia should be provided prior to carrying out an episiotomy, except in an emergency due to acute fetal compromise.
- Women with a history of severe perineal trauma should be informed that their risk of repeat severe perineal trauma is not increased in a subsequent birth, compared with women having their first baby.
- Episiotomy should not be offered routinely at vaginal birth following previous third- or fourth-degree trauma.
Third Stage of Labour
Definitions:
- Third stage of labour: the time from the birth of the baby to the expulsion of the placenta and membranes.
- Prolonged third stage: over 30 minutes
Observations
- Blood pressure and pulse
- Woman’s general physical condition, as shown by her colour, respiration and her own report of how she feels
- Vaginal blood loss
Recommendation
- Active management of the third stage is recommended, which includes the use of oxytocin (10 international units [IU] by intramuscular injection), followed by early clamping and cutting of the cord and controlled cord traction.
- Women should be informed that active management of the third stage reduces the risk of maternal haemorrhage and shortens the third stage.
- Pulling the cord or palpating the uterus should only be carried out after administration of oxytocin as part of active management.
- Start completing Postnatal Notes (Appendix 10)
Immediate Cord Care After Birth
- When the child the cord pulses and is fat and blue, do not cut at this time.
- Gently wipe the lochia off the baby and place on the mothers chest wrapped in a warm blanket.
- After a while, the cord will become thin and white, and stops pulsing.
- Wash hands thoroughly and use sterile gloves for the procedure.
- Tie the cord with clean or sterile string in two places: one 2 cm from the baby and 8 cm from the baby.
- Cut the cord closer to the baby about 2 cm from the first string using a sterile razor blade or scissors.
Indications for Transfer to More Advanced Healthcare Facility via Ambulance
- Need for continuous electronic fetal monitoring or EFM, indicated by:
- Significant meconium-stained liquor, and this change should also be considered for light meconium-stained liquor
- Abnormal FHR detected by intermittent auscultation: less than 110 beats per minute, greater than 160 bpm, any decelerations after a contraction; or uncertainty of presence of fetal heartbeat
- Maternal pyrexia: 38.0C once or 37.5C on two occasions 2 hours apart
- Fresh bleeding starting in labour
- Oxytocin use for augmentation of labour
- The woman’s request to be transferred
- Delay in the first or second stages of labour, diagnosed by:
- Cervical dilatation of less than 2 cm in 4 hours for first labour
- Cervical dilatation of less than 2 cm in 4 hours or a slowing in the progress of labour for second or subsequent labours
- Changes in the strength, duration and frequency of uterine contractions.
- Request for epidural pain relief
- Obstetric emergency – antepartum haemorrhage, cord presentation/prolapse, postpartum haemorrhage, maternal collapse or a need for advanced neonatal resuscitation
- Retained placenta that cannot be extracted by manual intervention
- Malpresentation or breech presentation diagnosed for the first time at the onset of labour, taking into account imminence of birth
- Either raised diastolic blood pressure: over 90 mmHg; or raised systolic blood pressure: over 140 mmHg; on two consecutive readings taken 30 minutes apart
- Third- or fourth-degree tear or other complicated perineal trauma requiring suturing
- If premature rupture of membranes occurred over 24 hours before onset of labour
Care of Mother and Baby Immediately After Birth
Care of baby
- APGAR scores at 1 and 5 minutes should be recorded for all births (See Appendix 11)
- If no respirations, stimulate baby, if stimulation ineffective, begin neonatal resuscitation, see Newborn Resuscitation Guidelines (Appendix 12).
- Obtain baby’s vital signs, see Newborn Vital Signs Guideline (Appendix 11).
- Skin-skin contact as soon as possible after birth
- Baby dried and covered in warm dry blanket
- Initial breastfeeding should be as soon as possible (within 1 hour of birth)
- Measurement of head circumference, body temperature and birth weight should be measured soon after the 1st hour
- An examination of the baby should be carried out to ensure no physical abnormality
- Apply Erythromycin ointment 0.5-1% or Tetracycline ointment 1% to both eyes within 1 hour of birth
- Administer Vitamin K 0.5 mg IM, within 1 hour of birth
- Complete Postnatal Notes (Appendix 10)
- Administer BCG immunisation prior to discharge, see Immunisation Guidelines (Appendix 21)
- Needs haemoglobin check before discharge
Care of woman
- Measure temperature, pulse, blood pressure, uterine contractions, lochia
- Examine placenta and membranes: assessment of their condition, structure, cord vessels and completeness
- Early assessment of maternal emotional/psychological condition
- Record successful voiding of the woman’s bladder within 6 hours post delivery
- Perineum Assessment and Repair (Appendix 13)
- Complete Postnatal Notes (Appendix 10)
Mothers who arrive in the immediate postnatal phase
- Ensure patient has been known to Chisang Clinic during the antenatal period, has attended all the required antenatal appointments and has had all the necessary investigations
- If not, then immediately send mother and baby to nearest hospital via emergency transportation
- If patient known to Chisang Clinic, then begin assessment of mother and baby
- Please refer to section a) Care of baby and section b) Care of woman above and follow recommended management plan
- If vital signs and observations within normal limits, mother and baby may stay at clinic for further management
- If any of the following occur, mother and baby should be transferred to nearest hospital
- Maternal systolic blood pressure greater than 140, less than 90, or diastolic blood pressure greater than 90
- Postpartum haemorrhage, with blood loss greater than 500 ml. See Management of Postpartum Haemorrhage (Appendix 19).
- Maternal collapse
- Maternal Pyrexia, defined by a temperature of 38C or greater
- Retained placenta
- Third or fourth degree perineal tear
- Abnormality of baby
- Neonatal resuscitation required at any point
- Please ensure patient and baby stabilized before transferring to hospital e.g. IV cannula inserted, fluid resuscitation
Postnatal Care
Postnatal Care of the Mother
- Please complete Initial Mother Assessment form in Postnatal Notes (Appendix 10)
- Give oral and demonstrational teaching on breastfeeding within 24 hours of birth, prior to discharge from birthing centre
- See General Postpartum Advice (Appendix 18)
Breastfeeding:
- See Breastfeeding Guidelines (Appendix 14) and Breastfeeding Poster
Danger Signs after Giving Birth
- See Danger Signs after Giving Birth (Appendix 15)
- See Danger Signs in the Newborn (Appendix 20)
Perineal Care
- Assess mother for perineal pain, discomfort or stinging, offensive perineal odour or dyspareunia.
- If the mother is experiencing discomfort, she should be taught that topical cold therapy provides effective perineal pain relief.
- Encourage perineal hygiene, such as frequent sanitary pad changes, frequent hand washing, and daily bathing to keep the perineum clean.
General Advice
- See Keeping Healthy After Giving Birth (Appendix 16)
Postnatal Care of the Baby
- Complete Initial Baby Assessment form in Postnatal Notes (Appendix 10)
- Complete full body assessment of baby, if any gross abnormalities, especially jaundice, within first 24 hours, baby may need to be referred to hospital of choice
Prior to Discharge
- Provide mother with chance to ask any questions she may have before leaving the clinic.
- Provide mother with documentation and help if necessary to fill out the appropriate government forms to be reimbursed for the delivery of her baby.
Postnatal Follow Up
Appointment at First Week
Follow Up for the Mother
- Ask about any issues experienced since birth, including the following problems:
– See Danger Signs After Giving Birth (Appendix 15)
– Signs of mastitis: flu-like symptoms, red, tender and painful breasts, if present, encourage gentle massage of breast, continued feeding, paracetamol for discomfort and increased fluid intake
– Constipation and haemorrhoids: if no bowel movement three days after birth, give patient a gentle laxative, encourage increased dietary fibre and fluid consumption in both cases, and encourage cold packs and paracetamol for pain management
– Urinary incontinence: if this is an issue, give teaching on Keagel exercises
– Fatigue: if experiencing excessive fatigue, review birthing events and antepartum history, if any signs indicate haemorrhage, check mother’s haemoglobin. If no indication for blood test, provide teaching on Keeping Healthy After Giving Birth, Appendix 16
– Emotional wellbeing: encourage the mother to communicate any changes in mood, emotional state or behaviour that seem abnormal to her
- Discuss plans for contraception following birth and encourage the mother to abstain from sexual intercourse for six weeks postpartum
Follow Up for the Baby
- Babies should be assessed for: temperature, heart rate, respiratory rate, colour, regular urination and stooling, general appetite and breast milk intake, body tone, and irritability.
- Assess for jaundice, pale stools and dark urine. If present assess severity, if acute jaundice present, refer to hospital.
Appointment at Sixth Week
Follow Up for the Mother
- Ask about any new health concerns and review the danger signs and questions asked in the first week postpartum to ensure no new concerns present
- Discuss the resumption of sexual intercourse and ask about any dyspareunia. If present, encourage water-based gel as lubricant during intercourse
Follow Up for the Baby
- Perform a complete physical assessment of the baby, as outlined in the Complete Physical Assessment of the Baby (Appendix 17) and assess social smiling and visual fixing at this time as well.
- Ask about any concerns the mother has had about her child since the last appointment
- Administer OPV and DPT immunisations, see Immunisation Guidelines (Appendix 21)
Appointment at Tenth Week
Follow Up for the Mother
- Ask about any concerns the mother has had since the previous appointment
- Continue to manage concerns that have arisen previously
Follow Up for the Baby
- Ask about any concerns the mother has had about the child since the last appointment
- Continue to manage concerns that have arisen previously
- Measure and plot height and weight on growth chart
- Administer OPV and DPT immunisations, see Immunisation Guidelines (Appendix 21)
Appointment at Fourteenth Week
- Administer OPV and DPT immunisations to baby, see Immunization Guidelines (Appendix 21)
Appointment at Sixth Month
- Measure and plot baby’s height and weight in growth chart
Appointment at Ninth Month
- Administer Measles immunisation to baby, see Immunisation Guidelines (Appendix 21)
Appointment at Twelfth Month
- Measure and plot baby’s height and weight in growth chart
- Administer Japanese Encephalitis immunisation to baby, see Immunisation Guidelines (Appendix 21)
Recommendations
- Input from O&G consultant from Nepal and overseas, a nurse midwife from Nepal and overseas before implementation
- Financial analyst to ascertain costs of project, including looking over the reimbursement forms for the clinic and mother
- Needs assessment for emergency vehicle for Birthing Centre
- Detailed discussion with Skilled Birthing Attendant to answer the following questions:
– Do they perform routine amniotomies?
– Are they trained in episiotomy and perineal repair?
– Do they manage 3rd and 4th degree perineal tears?
– What analgesia do they routinely use?
– Can they perform operative deliveries e.g. use vontouse and forceps
– Do they use active management of third stage of labour
– Do they manually remove placenta?
– Do they manage nulliparous women at a community birthing centre?
- Visit a similar birthing centre in Nepal
- Translate all documentation in Feasibility Study and Appendices into Nepali and adjust where culturally relevant
- Obtain Nepal guidelines for routine births and standards of care
- Obtain schedule of immunizations from Nepali government
- Obtain government educational materials e.g. posters and leaflets
- Obtain partogram
- Obtain guidelines for Oral Glucose Tolerance Test
Corinna Heiberg’s Public Health Perspective (Vol. II)
In my final semester at Berkeley before interning at Chisang Clinic I gave a presentation on uterine prolapse to a group of graduate students. Standing before the class I nervously repeated the lines I had already practiced countless times, saying “Uterine prolapse is a serious reproductive health condition that occurs when the uterus descends out of its usual position and falls out of the vagina. It has been estimated that approximately 200,000 women of all ages in Nepal are currently in need of immediate surgical treatment. Many of these women are unable to access medical care to get diagnosed or treated, and live for years with various symptoms that seriously affect their quality of life.” Though I had read extensively about UP in articles and online publications for classes before traveling to Nepal, I was not prepared and didn’t expect the number of women suffering from UP that I would meet in the village willing to candidly tell me their story. I was deeply affected by what I heard, and decided to share to raise awareness and reduce stigma surrounding the issue.
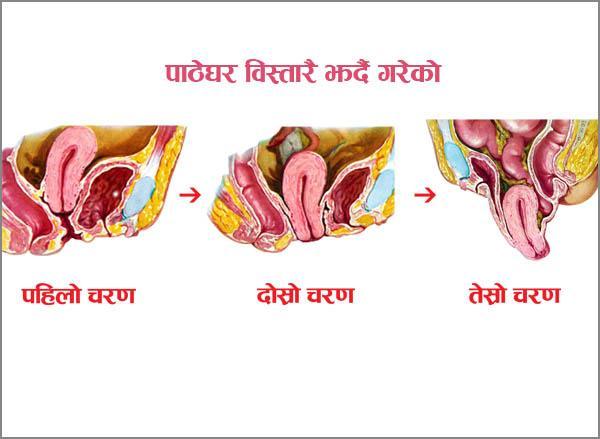
I met Nirmala, a young and energetic 28 year old woman, during my first week at the clinic. Over the summer all of the interns grew to love her and her eight year old son as they frequently stopped by just to chat and help out with anything the clinic needed. I came to find out that she had come into the clinic months earlier explaining that she felt as though “something is falling out when she strains”, finally revealing something she had kept secret for years. Through interviews and examinations I found out that since her son’s birth, which occurred at home before she was rushed to the hospital for post partum hemorrhage, she has suffered from many of the symptoms of UP, including irregular menstruation, stress incontinence, painful intercourse, and pain sitting, walking or riding a bicycle. It has also affected her ability to work in the fields, her relationship with her husband, and her ability to interact with the community. She is only in the early stages of anterior wall prolapse and doesn’t yet need a hysterectomy, but the clinic does not have the facilities or medical supplies at this time to provide treatment. Though the clinic could not help her physically without more resources, she was extremely relieved that she finally had people to talk to and could receive some counseling about home remedies and exercises she could try.

I also met women like Rita, a 67 year old woman with severe pain and the feeling of “something coming down” her vagina. Rita is more characteristic of women suffering from uterine prolapse because she had six children all born at home at a very young age. A combination of these factors likely led to her anterior uterine wall falling down and many debilitating symptoms. Unlike Nirmala, she was very ashamed by her condition, and agreed to an examination only after lengthy discussion and reassurance, though she remained visibly distressed and uncomfortable. Without the privacy and accessibility of the clinic, it is likely that she would never have had the confidence to seek medical care.

These two women, along with the others who came to Chisang Clinic seeking relief from the symptoms of uterine prolapse, cited many potential causes for their condition, such as strenuous manual labor, lack of trained assistance during delivery, lack of post-partum rest, and inadequate spacing between births. Most of these are completely preventable. The Clinic is working to increase awareness about the risks of prolapse, but unfortunately at this time has neither the surgeons nor resources to help the women, and no knowledge of facilities near enough to refer women that are accessible and affordable. The birthing center is a great first step at preventing future uterine prolapse cases by providing facility births, administering a checklist developed to screen patients, and increasing counseling about uterine prolapse during routine ANC and gynecological visits. The clinic also welcomes any aid in setting up a temporary uterine prolapse clinic with trained medical professionals who could provide treatment for women in the area and train the clinic staff to insert pessaries. With some outside help, the clinic has a great opportunity to improve the lives of countless women in Bhaunne and many other regions of Nepal.













Corinna Heiberg’s Public Health Perspective (Vol. I)
On a hot, humid summer day during my first month at Chisang Clinic, I biked behind Anita and Gita, trying to keep up as they navigated the narrow dusty roads of the village. Using a hand drawn map we had made plotting the home of every woman in Bhaunne who was either pregnant or had recently given birth, we quickly arrived at the first home. I apprehensively followed the two staff inside, carrying the list of questions I had developed regarding women’s age at marriage, pregnancy, and childbirth. After sitting down on the patio, drinking some delicious chiya (milk tea), and listening to the girls chat at length with Sushila, I began to ask my questions. Sushila immediately opened up, elaborating on her responses and telling me stories about her life. Like the majority of women who I interviewed, Sushila was married at a young age, had never previously used contraceptives, had her first child within a year of marriage, and had her first two children at home with no medical attendant. Sushila’s candidacy gave me an eye-opening glimpse into the challenges many Nepali women face accessing quality healthcare.


In the following weeks I biked to over fifty women’s homes asking the same questions as part of an informal research project I had developed based on my interest in Maternal and Child Health. As a recent public health graduate, this opportunity to conduct inquiries in the community gave me a different experience than the two previous medical interns at the clinic who primarily worked in the examination room checking patients and prescribing medications. My aim was to identify health seeking behaviors and services available for women in the village by addressing issues about the quality of antenatal care and choices made about contraception and birthing. Due to the relationship the Clinic had already established with the local community, I was given direct access into the women’s homes. I was also provided with all of the resources and assistance by the dedicated staff, who accompanied me on every home visit, helped me find the women’s homes, and translated all of my questions.
 Though the primary aim of my home visits was to use women’s responses about pregnancy and childbirth in the design of the new birthing center, I learned about many other women’s health issues that the clinic was able to address. For example, I discovered over the course of the interview that Sushila’s third child had been an unplanned pregnancy and she was interested in using some form of contraceptives. I recommended that she consider coming in to the clinic to try Depo, and I was extremely happy and proud when she ended up being one of our first patients seeking family planning services.
Though the primary aim of my home visits was to use women’s responses about pregnancy and childbirth in the design of the new birthing center, I learned about many other women’s health issues that the clinic was able to address. For example, I discovered over the course of the interview that Sushila’s third child had been an unplanned pregnancy and she was interested in using some form of contraceptives. I recommended that she consider coming in to the clinic to try Depo, and I was extremely happy and proud when she ended up being one of our first patients seeking family planning services.
In Bhaunne there is high demand for this injectable form of contraception, largely due to the fact that it is a highly effective, private, easy, and reversible way for women of reproductive age to control their fertility and achieve their desired family size. After developing Depo forms to log women’s visits and buying the necessary injection supplies, Chisang Clinic was finally able to offer family planning services on July 3rd! Unlike in the pharmacies, where women are quickly injected by someone with only a couple months training, Chisang Clinic staff do a formal screening of each woman, provide advice regarding the side effects, and give more extensive one-on-one counseling for women like Sushila.

 During the rest of my time at the Clinic the women who came in for Depo were often times the women I had spoken with, who had recently given birth and were seeking a way to either create a “gap” before their second child or prevent any further pregnancies. These women also came in for routine check ups and brought their newborns in when they were sick, showing that there was a definite demand in the community for the services that the Clinic provided. When Chisang Clinic opens the birthing center hopefully even more gynecological and obstetric services will be available, so every women can not only come in for family planning services, but also for STD testing, pap smears, and giving birth to their child.
During the rest of my time at the Clinic the women who came in for Depo were often times the women I had spoken with, who had recently given birth and were seeking a way to either create a “gap” before their second child or prevent any further pregnancies. These women also came in for routine check ups and brought their newborns in when they were sick, showing that there was a definite demand in the community for the services that the Clinic provided. When Chisang Clinic opens the birthing center hopefully even more gynecological and obstetric services will be available, so every women can not only come in for family planning services, but also for STD testing, pap smears, and giving birth to their child.
Giovanna DeLuca’s Chisang Clinic Experience (Vol. I)
The Road from Biratnagar to Chisang Clinic
As I’m waiting at baggage claim, and by baggage claim I mean a room about the size of my living room where a man comes and drops your bags on a table for people to sort through, a small man named Kewal comes up behind me and says ‘Chisang Clinic?’ “Yes!” I found my driver, or he found me, which was probably more difficult than he imagined because my brown skin and Asian eyes have allowed me to blend in quite well. We load my backpack and my suitcase full of medical supplies on the back of his colorful little van and drive off.
If anything will make you fall in love with Nepal, it is the road from Biratnagar to Chisang Clinic. Along the sides of this national highway are cows, goats, chickens, people carrying hay on their heads, bicyclists, school children, palm trees, bamboo trees, huts, pastel houses, women in beautiful colorful dresses, all set in front of a mountainous green background where the clouds are so low you’d think you could reach up and grab one. I had learned in India that is it polite to honk a couple times at each car, some buses and trucks even have “Please Honk” painted on the their backsides. It seems to be the same here. Although it is a two way street no one seems to pay attention to the divider line and vehicles swerve all over the road. The only rule there seems to be is ‘don’t hit anything’. I guess that’s where the honking comes in…to let everyone know your coming. Through the madness I feel calm and much less frightened than I should. Kewal seems to know what he is doing and I imagine he could troll the streets of New York better than any New Yorker. I’m so fascinated that the the supposed hour long ride seems to go by in 5 minutes as Kewal pulls off onto a dirt road and the cars seem to lessen and the animals seem to grow in abundance. Eventually the car slows down and then comes to a stop. We have arrived.

A Rickshaw in Biratnaagar

“Honk Please”

Roadside Houses on the Way to Bhaunee

Baggage Claim at the Biratnagar Domestic Airport
Dr Briana’s Village Pictures

Anita and her grandmother at Bhaunne

Village woman carries fodder for her goats

Clinic Electrician Jhalendra with his son, Shishir

A Traditional Choir Specializing in Singing Bhajans (Traiditional Hindu Hymns)

Dr Briana examines an elderly lady at her home at Sabhapur

Community Outreach at Shabhapur

Bhaunne children pose for a picture with their grandmother

A 70 year old Stilt House at Bhaunne

Clinic neighbor drying rice in preparation to cook celroti

Dr Briana ponding rice to make flour

Clinic neighbors take turn pounding rice

Another Bhaunne family pose for a picture

Dr Briana with Anita’s grandmother
